Project Malnutrition
Innovation for Africa’s Malnutrition Crisis

Duration
6 months / 2015 - 16
Client
International Rescue Committee
Role
Service design
Design research
Prototyping
Team
Quicksand Design Studio
6 months / 2015 - 16
Client
International Rescue Committee
Role
Service design
Design research
Prototyping
Team
Quicksand Design Studio
Project Malnutrition aimed at developing and delivering a new set of tools to identify & monitor severe acute malnutrition amongst children across several African countries.
A key mandate of the project was to ensure that the tools could be used by healthcare workers lacking literacy or numeracy, and that the same system of tools could be scaled and deployed across all countries in Africa where the IRC works.
A final toolkit, along with a detailed training manual for the use of composite artefacts was field tested in South Sudan and delivered for deployment across IRC’s nutrition program in Africa.
All the material within this section is copyrighted to Quicksand Design Studio.




IRC had identified South Sudan as the most challenging context for its nutrition programme. The technical team at IRC supported this project.
As a design associate, I was responsible for research, product explorations and supporting the inclusion of designed artefacts within the overall service design.
The system of tools went through first round of testing and validation in India. The final version was tested in South Sudan before the delivery and deployement of the toolkit.

Process
1/ Explorations
2/ Local Testing
3/ Field Testing


1/
Explorations
In many African villages, a distributed system of providing healthcare has emerged due to limited resouces and manpower.
Within villages, community based distributors or CBDs are responsible for assessing young children with signs of malnourishment and distributing health supplements needed to counter it.
Within villages, community based distributors or CBDs are responsible for assessing young children with signs of malnourishment and distributing health supplements needed to counter it.
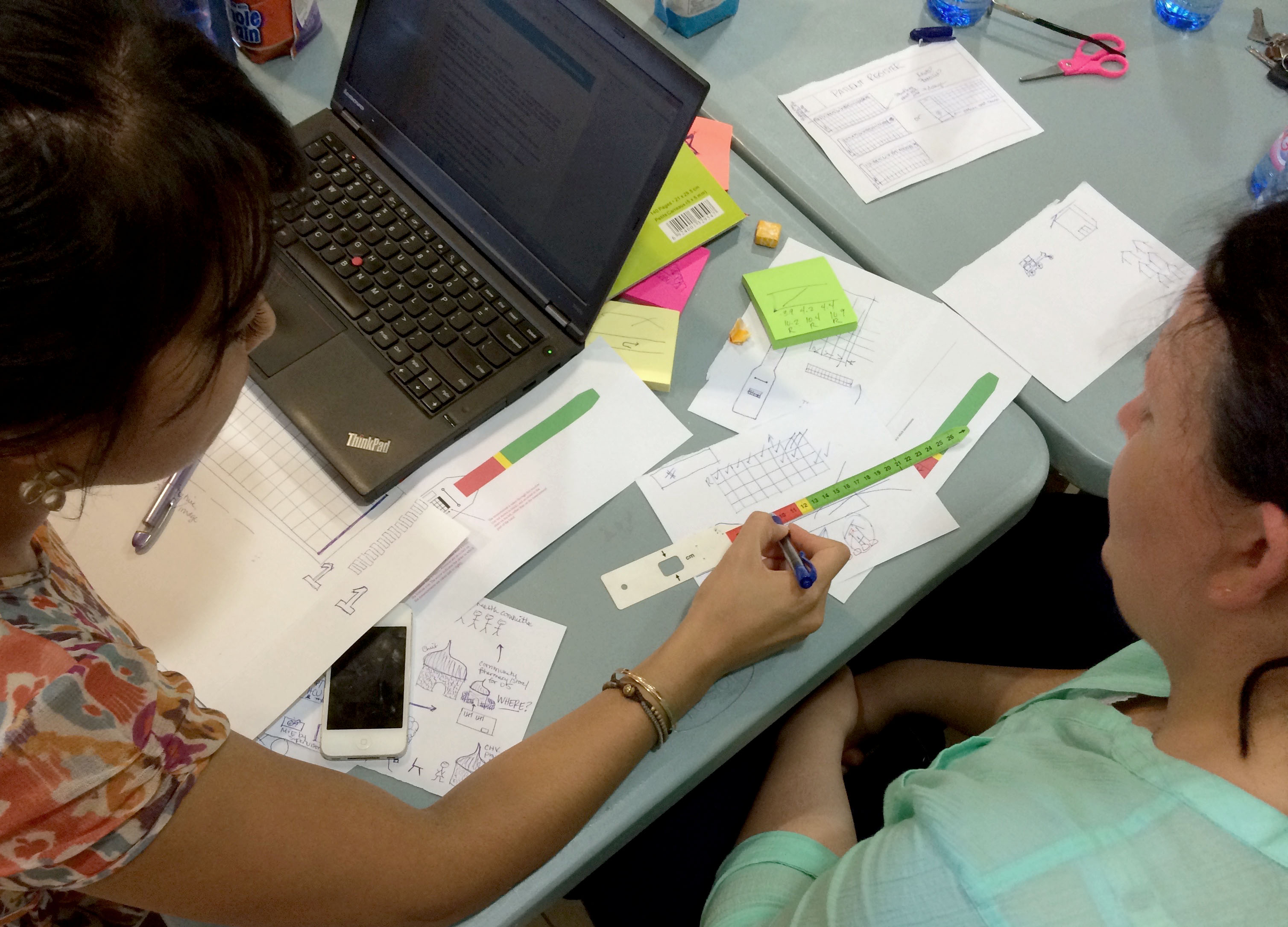
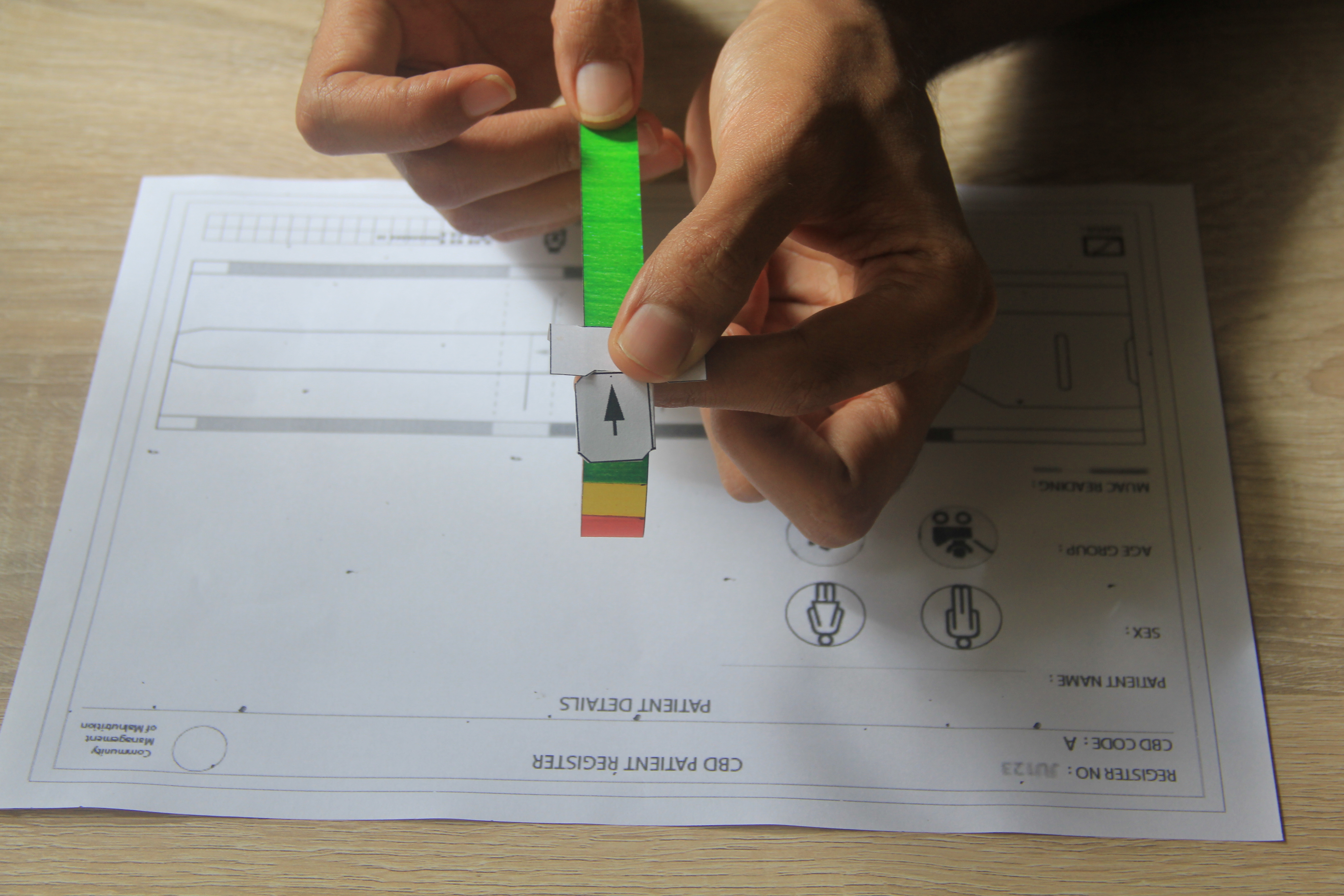
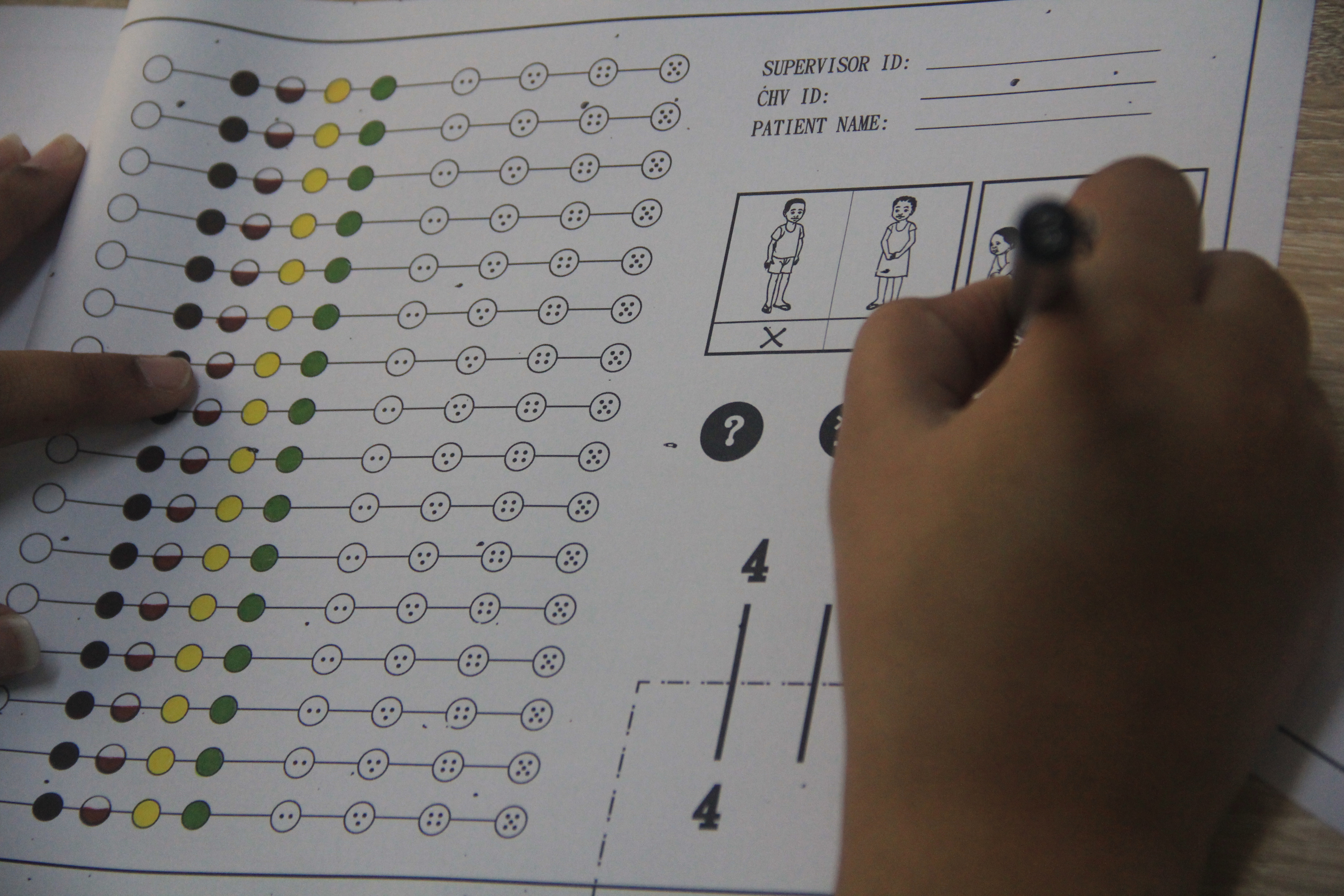
In order to assess and track the signs of malnutrition, the CBDs use three main elements: a MUAC tape, a register, and a weight measurement.
Our team’s main challenge was to design these in such a way that they can be operated without literacy or numeracy. The following images show some explorations.
Our team’s main challenge was to design these in such a way that they can be operated without literacy or numeracy. The following images show some explorations.




2/
Local testing
Before taking the tools and the manuals for a field testing in South Sudan, they were tested and validated within a health clinic set-up in the city of Bhopal in central India.
Like the community based distributors, the healthworkers within this clinic had similar roles and responsibilties, and were able to share their experiences and give feedback on the use of the toolkit and manuals.

3/
Field testing
The final tools were re-designed and produced for field testing in South Sudan.
Two members of the our project team travelled to a small village in South Sudan where they were able to interact with the community based distributors and learn about their experiences and incorporate their reflections to refine the toolkit.
Two members of the our project team travelled to a small village in South Sudan where they were able to interact with the community based distributors and learn about their experiences and incorporate their reflections to refine the toolkit.

